- About
- Mission Statement
Education. Evidence. Regrowth.
- Education.
Prioritize knowledge. Make better choices.
- Evidence.
Sort good studies from the bad.
- Regrowth.
Get bigger hair gains.
Team MembersPhD's, resarchers, & consumer advocates.
- Rob English
Founder, researcher, & consumer advocate
- Research Team
Our team of PhD’s, researchers, & more
Editorial PolicyDiscover how we conduct our research.
ContactHave questions? Contact us.
Before-Afters- Transformation Photos
Our library of before-after photos.
- — Jenna, 31, U.S.A.
I have attached my before and afters of my progress since joining this group...
- — Tom, 30, U.K.
I’m convinced I’ve recovered to probably the hairline I had 3 years ago. Super stoked…
- — Rabih, 30’s, U.S.A.
My friends actually told me, “Your hairline improved. Your hair looks thicker...
- — RDB, 35, New York, U.S.A.
I also feel my hair has a different texture to it now…
- — Aayush, 20’s, Boston, MA
Firstly thank you for your work in this field. I am immensely grateful that...
- — Ben M., U.S.A
I just wanted to thank you for all your research, for introducing me to this method...
- — Raul, 50, Spain
To be honest I am having fun with all this and I still don’t know how much...
- — Lisa, 52, U.S.
I see a massive amount of regrowth that is all less than about 8 cm long...
Client Testimonials150+ member experiences.
 Scroll DownPopular Treatments
Scroll DownPopular Treatments- Treatments
Popular treatments. But do they work?
- Finasteride
- Oral
- Topical
- Dutasteride
- Oral
- Topical
- Mesotherapy
- Minoxidil
- Oral
- Topical
- Ketoconazole
- Shampoo
- Topical
- Low-Level Laser Therapy
- Therapy
- Microneedling
- Therapy
- Platelet-Rich Plasma Therapy (PRP)
- Therapy
- Scalp Massages
- Therapy
 More
More
IngredientsTop-selling ingredients, quantified.
- Saw Palmetto
- Redensyl
- Melatonin
- Caffeine
- Biotin
- Rosemary Oil
- Lilac Stem Cells
- Hydrolyzed Wheat Protein
- Sodium Lauryl Sulfate
 More
More
ProductsThe truth about hair loss "best sellers".
- Minoxidil Tablets
Xyon Health
- Finasteride
Strut Health
- Hair Growth Supplements
Happy Head
- REVITA Tablets for Hair Growth Support
DS Laboratories
- FoliGROWTH Ultimate Hair Neutraceutical
Advanced Trichology
- Enhance Hair Density Serum
Fully Vital
- Topical Finasteride and Minoxidil
Xyon Health
- HairOmega Foaming Hair Growth Serum
DrFormulas
- Bio-Cleansing Shampoo
Revivogen MD
- more
Key MetricsStandardized rubrics to evaluate all treatments.
- Evidence Quality
Is this treatment well studied?
- Regrowth Potential
How much regrowth can you expect?
- Long-Term Viability
Is this treatment safe & sustainable?
Free Research- Free Resources
Apps, tools, guides, freebies, & more.
- Topical Finasteride Calculator
- Interactive Guide: What Causes Hair Loss?
- Free Guide: Standardized Scalp Massages
- 7-Day Hair Loss Email Course
- Ingredients Database
- Interactive Guide: Hair Loss Disorders
- Treatment Guides
- Product Lab Tests: Purity & Potency
- Evidence Quality Masterclass
- More
Articles100+ free articles.
-
Cannabidiol (CBD) Increases Hair Counts By 246%? Not So Fast.
-
Creatine: Does It Worsen Hair Loss? It Depends On The Hair Loss Type.
-
Can Progesterone Improve Hair Regrowth?
-
CRABP2: Can This Gene Predict Regrowth From Retinoids?
-
BTD: Can This Gene Predict Regrowth From Biotin?
-
COL1A1: Can This Gene Predict Regrowth From Collagen Support?
-
2dDR For Hair Loss: What Do We Know So Far About This Sugar?
-
CYP19A1: Can This Gene Predict Regrowth From Hormone Therapy?
PublicationsOur team’s peer-reviewed studies.
- Microneedling and Its Use in Hair Loss Disorders: A Systematic Review
- Use of Botulinum Toxin for Androgenic Alopecia: A Systematic Review
- Conflicting Reports Regarding the Histopathological Features of Androgenic Alopecia
- Self-Assessments of Standardized Scalp Massages for Androgenic Alopecia: Survey Results
- A Hypothetical Pathogenesis Model For Androgenic Alopecia:Clarifying The Dihydrotestosterone Paradox And Rate-Limiting Recovery Factors
Menu- AboutAbout
- Mission Statement
Education. Evidence. Regrowth.
- Team Members
PhD's, resarchers, & consumer advocates.
- Editorial Policy
Discover how we conduct our research.
- Contact
Have questions? Contact us.
- Before-Afters
TreatmentsOral Dutasteride
Evidence59%RegrowthViabilityTopical Dutasteride
Evidence55%RegrowthViabilityMesotherapy Dutasteride
Evidence60%RegrowthViability-
Oral
-
Topical
-
Mesotherapy
-

Evidence Quality
59%
Regrowth Potential
Long-Term Viability
Written by Perfect Hair Health TeamMedically Reviewed by Rob EnglishFirst Published Oct 2, 2024Last Updated Oct 23, 2024Key Information
Free Resources
KEY INFORMATIONWhat Is Dutasteride?
Dutasteride is a drug that lowers dihydrotestosterone (DHT) – a hormone causally linked to androgenic alopecia. Dutasteride is FDA-approved to treat benign prostatic hyperplasia, but is also prescribed off-label for hair loss in oral, topical, and mesotherapy formulations.
How Does Dutasteride Work?
Dutasteride lowers DHT by inhibiting type I and II 5-alpha reductase. At daily doses of 0.5 mg and higher, dutasteride can reduce DHT by 90% and more.
What You Should Know
Clinical studies show that dutasteride reduces more DHT and grows more hair than finasteride. Despite this, dutasteride has no increased risk versus finasteride for sexual side effects. Interestingly, topical dutasteride is well-tolerated by members here who experienced side effects on topical finasteride – with some members showing no changes to serum DHT at applications up to 6 mg weekly of topical dutasteride.
-

Evidence Quality
55%
Regrowth Potential
Long-Term Viability
Written by Perfect Hair Health TeamMedically Reviewed by Rob EnglishFirst Published Oct 2, 2024Last Updated Oct 23, 2024Key Information
Free Resources
KEY INFORMATIONWhat Is Dutasteride?
Dutasteride is a drug that lowers dihydrotestosterone (DHT) – a hormone causally linked to androgenic alopecia. Dutasteride is FDA-approved to treat benign prostatic hyperplasia, but is also prescribed off-label for hair loss in oral, topical, and mesotherapy formulations.
How Does Dutasteride Work?
Dutasteride lowers DHT by inhibiting type I and II 5-alpha reductase. At daily doses of 0.5 mg and higher, dutasteride can reduce DHT by 90% and more.
What You Should Know
Clinical studies show that dutasteride reduces more DHT and grows more hair than finasteride. Despite this, dutasteride has no increased risk versus finasteride for sexual side effects. Interestingly, topical dutasteride is well-tolerated by members here who experienced side effects on topical finasteride – with some members showing no changes to serum DHT at applications up to 6 mg weekly of topical dutasteride.
-

Evidence Quality
60%
Regrowth Potential
Long-Term Viability
Written by Perfect Hair Health TeamMedically Reviewed by Rob EnglishFirst Published Oct 2, 2024Last Updated Oct 23, 2024Key Information
Free Resources
KEY INFORMATIONWhat Is Dutasteride?
Dutasteride is a drug that lowers dihydrotestosterone (DHT) – a hormone causally linked to androgenic alopecia. Dutasteride is FDA-approved to treat benign prostatic hyperplasia, but is also prescribed off-label for hair loss in oral, topical, and mesotherapy formulations.
How Does Dutasteride Work?
Dutasteride lowers DHT by inhibiting type I and II 5-alpha reductase. At daily doses of 0.5 mg and higher, dutasteride can reduce DHT by 90% and more.
What You Should Know
Clinical studies show that dutasteride reduces more DHT and grows more hair than finasteride. Despite this, dutasteride has no increased risk versus finasteride or sexual side effects. Interestingly, topical dutasteride is well-tolerated by members here who experienced side effects on topical finasteride – with some members showing no changes to serum DHT at applications up to 6 mg weekly of topical dutasteride.
FREE RESOURCESArticles
Explore the science behind hair loss and hair growth. Our in-depth articles cover topics ranging from natural remedies to pharmaceuticals to breakthroughs in hair loss science. Want to request an article topic? Contact us.
 By Ben Fletcher, PhDAug 6, 2024
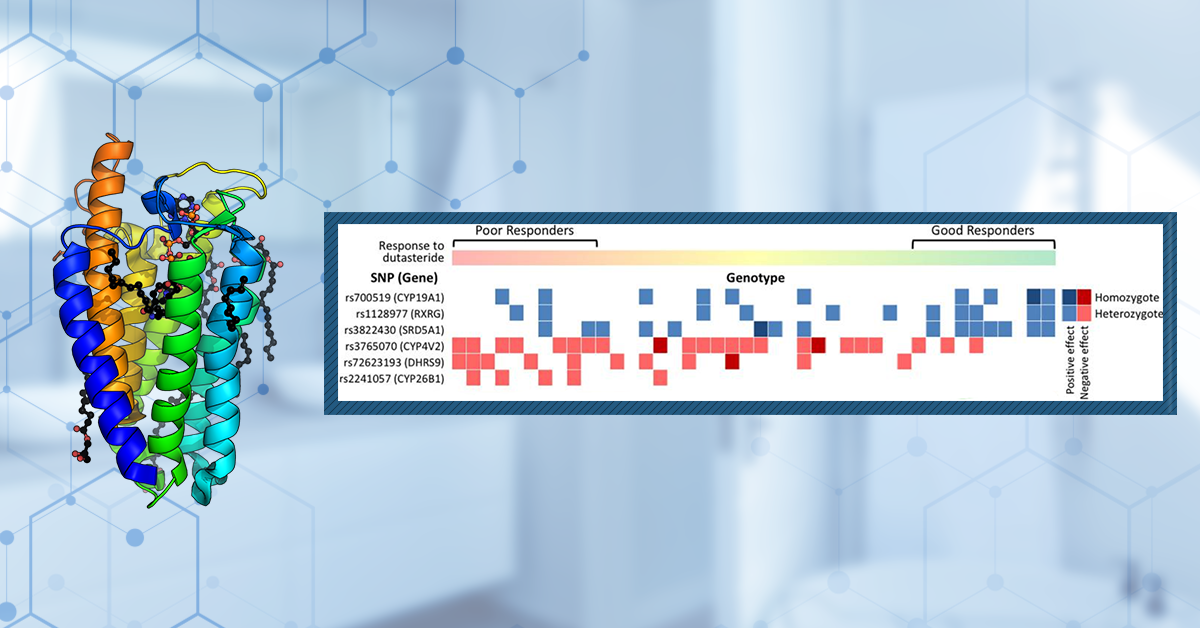
By Ben Fletcher, PhDAug 6, 2024SRD5A1 & 2: Can These Genes Predict Regrowth From 5-Alpha-Reductase Inhibitors?
Can your genes predict the effectiveness of 5α-reductase inhibitors for hair loss? The SRD5A1 and SRD5A2 genes, encoding type I and type II 5α-reductase respectively, are central to DHT production, a key factor in the pathogenesis of androgenic alopecia. Genetic testing companies suggest certain SR5...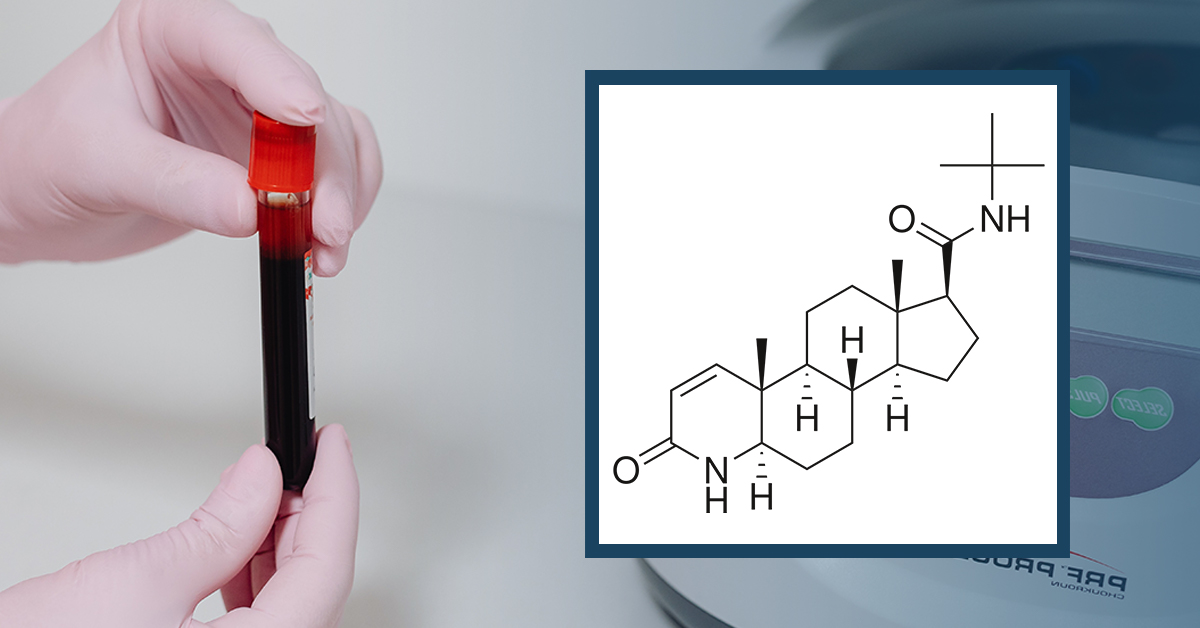 By Perfect Hair Health TeamJan 15, 2023
By Perfect Hair Health TeamJan 15, 2023Can a Blood Test for Finasteride Determine the Risk of Side Effects?
Can blood tests reliably determine the risk of sexual side effects from hair loss drugs? Low-quality evidence (i.e., anecdotes and observational studies) suggest, in men, that low levels of free testosterone and/or high levels of sex hormone binding globulin are correlated with higher rates of sexua...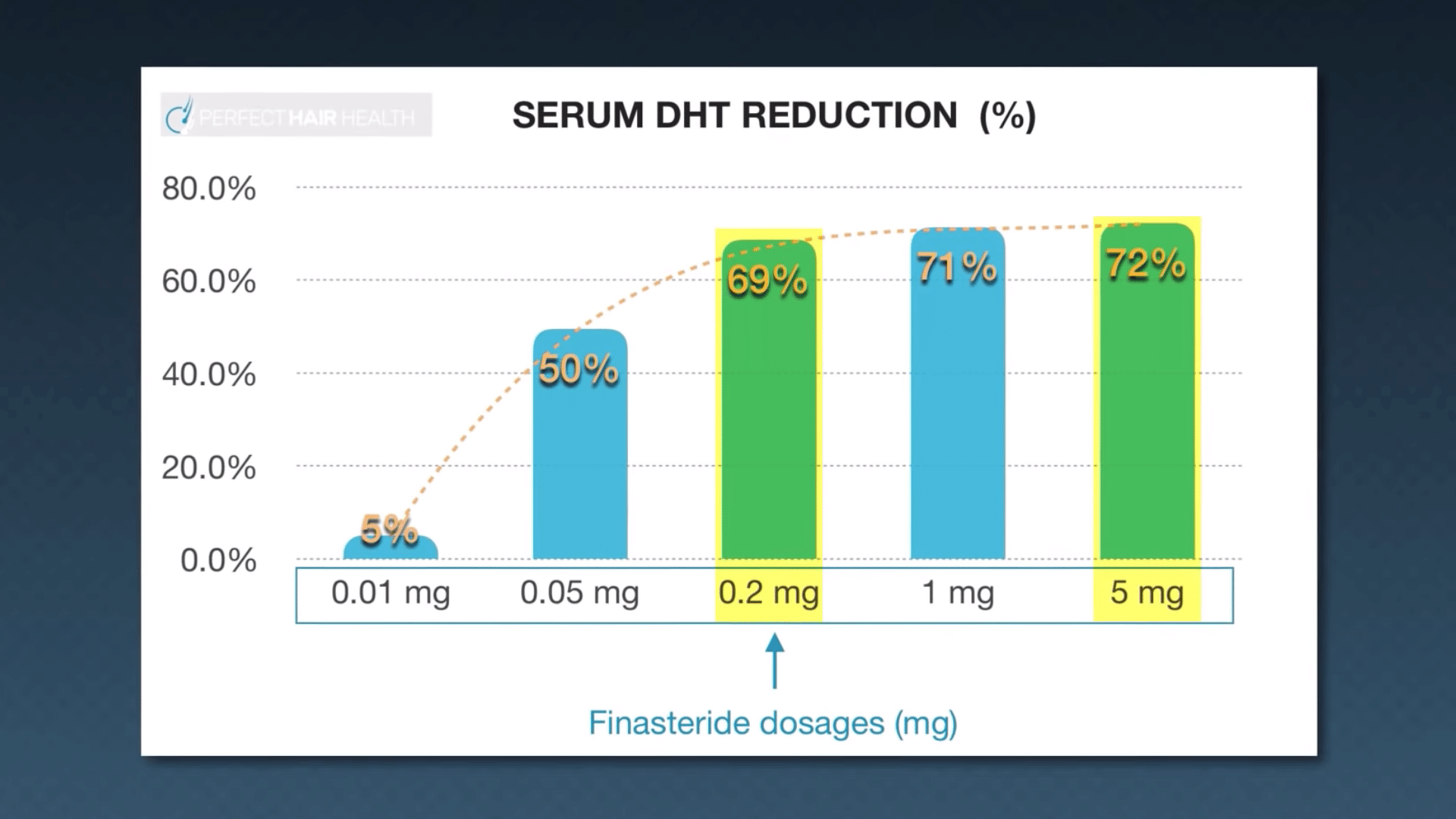 By Perfect Hair Health TeamApr 6, 2022
By Perfect Hair Health TeamApr 6, 2022The 6 Best DHT Blockers For Men
Which DHT blockers work? Which ones put hair loss sufferers at a greater risk of side effects? What does the actual evidence say versus marketing hype for the latest DHT-reducing supplements, topicals, and drugs? The answers may surprise you. In this article, the Perfect Health Team evaluates 6 DHT ...FREE RESOURCESArticles
Explore the science behind hair loss and hair growth. Our in-depth articles cover topics ranging from natural remedies to pharmaceuticals to breakthroughs in hair loss science. Want to request an article topic? Contact us.
By Ben Fletcher, PhDAug 6, 2024SRD5A1 & 2: Can These Genes Predict Regrowth From 5-Alpha-Reductase Inhibitors?
Can your genes predict the effectiveness of 5α-reductase inhibitors for hair loss? The SRD5A1 and SRD5A2 genes, encoding type I and type II 5α-reductase respectively, are central to DHT production, a key factor in the pathogenesis of androgenic alopecia. Genetic testing companies suggest certain SR5...
By Perfect Hair Health TeamJan 15, 2023Can a Blood Test for Finasteride Determine the Risk of Side Effects?
Can blood tests reliably determine the risk of sexual side effects from hair loss drugs? Low-quality evidence (i.e., anecdotes and observational studies) suggest, in men, that low levels of free testosterone and/or high levels of sex hormone binding globulin are correlated with higher rates of sexua...
By Perfect Hair Health TeamApr 6, 2022The 6 Best DHT Blockers For Men
Which DHT blockers work? Which ones put hair loss sufferers at a greater risk of side effects? What does the actual evidence say versus marketing hype for the latest DHT-reducing supplements, topicals, and drugs? The answers may surprise you. In this article, the Perfect Health Team evaluates 6 DHT ...FREE RESOURCESArticles
Explore the science behind hair loss and hair growth. Our in-depth articles cover topics ranging from natural remedies to pharmaceuticals to breakthroughs in hair loss science. Want to request an article topic? Contact us.
By Ben Fletcher, PhDAug 6, 2024SRD5A1 & 2: Can These Genes Predict Regrowth From 5-Alpha-Reductase Inhibitors?
Can your genes predict the effectiveness of 5α-reductase inhibitors for hair loss? The SRD5A1 and SRD5A2 genes, encoding type I and type II 5α-reductase respectively, are central to DHT production, a key factor in the pathogenesis of androgenic alopecia. Genetic testing companies suggest certain SR5...
By Perfect Hair Health TeamJan 15, 2023Can a Blood Test for Finasteride Determine the Risk of Side Effects?
Can blood tests reliably determine the risk of sexual side effects from hair loss drugs? Low-quality evidence (i.e., anecdotes and observational studies) suggest, in men, that low levels of free testosterone and/or high levels of sex hormone binding globulin are correlated with higher rates of sexua...-
FREE RESOURCES
Research Tables
Want the latest research on Oral Dutasteride? Every quarter, our research team conducts a literature search on Oral Dutasteride to keep you up-to-date on new studies. See our search criteria & research tables below – including a summary of key findings from every single study.
Last updated: October 2024
Results
Search Criteria
Parameter
Inclusion Criteria
Exclusion Criteria
Patients Patients of any age with hair loss. Patients with no hair loss disorder. Intervention Oral dutasteride as a standalone or adjunct therapy. A study that doesn’t contain oral dutasteride either as a standalone or adjunct therapy. Comparator Placebo and/or other therapies or baseline. No comparator. Outcomes Primary Endpoints of phototrichogram, investigator, and/or patient assessments. Any study not designed to adequately test for the standalone or additive effect of oral dutasteride. Study Design Prospective, observational, retrospective, and case series studies. Literature reviews, non-human subjects, or ongoing clinical trials. Search Terms
Search Terms:
oral hair loss alopecia dutasteride-
Abbreviations:
-
FFAFrontal Fibrosing Alopecia
-
AGAAndrogenetic Alopecia
-
DSTDutasteride
-
DHTDihydrotestosterone
Summarized Studies
Study Participants Design Treatment Results Key Takeaway Adverse Effects Evidence Quality Authors (year) Sex Hair Loss Type Design Dose Usage Duration Endpoints Hair Growth Assessments and Changes in Serum/Scalp DHT Summary Limitations Adverse Effects Jadad Score Vano-Galvan et al (2020) n=42 (m)
Group 1: 12
Group 2: 15
Group 3: 15 AGA
AGARetrospective, monocentric, descriptive study Group 1: less than 3 0.5 mg DST capsules/week
Group 2: 5 0.5 mg DST capsules/week
Group 3: 7 0/5 mg DST capsules/week.Weekly. 52 weeks minimum. Comparison of pre-and post-treatment with clinical images by 3 independent dermatologists using a 4-point scale. Group 1: 4/12 patients were stable, and 8/12 patients showed mild improvement.
Group 2: 11/15 patients showed mild improvement, 4/15 patients showed marked improvement.
Group 3: 9/15 patients showed mild improvement, 6/15 patients showed marked improvement.7 capsules of 0.5 mg DST appeared to lead to the highest number of patients who showed marked improvement. Retrospective study. Group 2: Erectile dysfunction (1), Decreased libido (1).
Group 3: Decreased libido (1).
None of these side effects caused withdrawal from the study.1Tsunemi et al (2016) n=110 (M) AGAMulticenter, open-label, prospective, outpatient study. All patients took 1 capsule of 0.5 mg DST. Once daily. 52 weeks. Hair growth, hair restoration, global improvement in hair and change in AGA stage, safety assessments. Mean target hair count:
Baseline: 87.3±81.14
Week 26: 72±102.6
Week 52: 68.1±82.14
Hair Width: Week 26: 6.7 μm±4.8
Week 52: 6.5 μm±5.29
Terminal Hair Count:
Week 26: 60.8±70.22
Week 52: 76.9±86.19
Investigator Assessment:
Week 52: Improvement was observed in 40% of patients who were at stage III vertex at baseline, 43% of patients who were at stage IV, and 84% of patients who were at stage V.
Serum DHT:
Week 26: -84.9% compared to baseline
Week 52: -85.4% compared to baseline.0.5 mg of DHT appears to exhibit good efficacy, safety, and tolerability. High variation in results, open-label design. Drug-related adverse events:
Erectile dysfunction (11%), libido decrease (8%), Ejaculation disorder (4%), sexual dysfunction (3%), retrograde ejaculation (<1), depressed mood (<1), suicidal ideation (<1), headache (<1), sensory disturbance (<1), fatigue (<1), rash (<1), hypertension (<1).1Stough (2007) n=34 (17 pairs of twins)
Group 1: 17
Group 2: 17AGAA randomized, placebo-controlled, double-blind study. Group 1: 0.5 mg
Group 2: placeboOnce daily 52 weeks. Standardized clinical photographs, Hair counts, and Patient self-assessment questionnaires. Change from Baseline - Hair Counts at 52 weeks:
Week 52:
Group 1: +16.5
Group 2: -3.8
Hair Growth Scores:
Week 52:
Group 1: 5 (slightly improved)
Group 2: 4.07 (no change)0.5 mg DST daily appears to improve hair counts and scores over a year of treatment. Small sample size. Group 1: decreased libido of mild to moderate severity (2). 3 -
-
FREE RESOURCES
Research Tables
Want the latest research on Topical Dutasteride? Every quarter, our research team conducts a literature search on Topical Dutasteride to keep you up-to-date on new studies. See our search criteria & research tables below – including a summary of key findings from every single study.
Last updated: October 2024
Results
Search Criteria
Parameter
Inclusion Criteria
Exclusion Criteria
Patients Patients of any age with hair loss. Patients with no hair loss disorder. Intervention Topical dutasteride as a standalone or adjunct therapy. A study that doesn’t contain topical dutasteride either as a standalone or adjunct therapy. Comparator Placebo and/or other therapies or baseline. No comparator. Outcomes Primary Endpoints of phototrichogram, investigator, and/or patient or physician assessments. None. Study Design Prospective, observational, retrospective, and case series studies. Literature reviews, non-human subjects, or ongoing clinical trials. Search Terms
Search Terms:
topical alopecia hair loss dutasteride-
Abbreviations:
-
MNMicroneedling
-
MXMinoxidil
-
DSTDutasteride
-
GPAGlobal Photographic Assessment
-
VASVisual Analog Scale
-
CIAChemotherapy-induced alopecia
-
FPHLFemale pattern hair loss
-
AGAAndrogenic alopecia
Summarized Studies
Study Participants Design Treatment Results Key Takeaway Adverse Effects Evidence Quality Authors (year) Sex Hair Loss Type Design Dose Usage Duration Endpoints Hair Growth Assessments and Changes in Serum/Scalp DHT Summary Limitations Adverse Effects Jadad Score Nada et al (2018) n=30 (M)
Group 1: 15
Group 2: 15AGAProspective, randomized, clinical study Group 1: MN + topical DST (0.02%)
Group 2: MN only13 sessions (once every week for 8 weeks, then once every two weeks for one month, then once every month for three months) 24 weeks Hair loss grading, phototrichoscopy (hair density, hair width, terminal/vellus hair ratio), patient self-assessment, investigator assessment, adverse effects, and hormone levels. Change in hair density:
Group 1: 27.6±62.49
Group 2: -9±30.30 (p=0.02)
Change in hair width:
Group 1: 0.023±0.024
Group 2: 0.0003±0.015 (p=0.003)
Change in terminal/vellus ratio:
Group 1: 3.10±6.17
Group 2: 0.17±1.40 (p=0.02)
Patient self-assessment: Higher ‘improvement’ and ‘satisfaction’ scores in Group 1 than in Group 2.
Change in serum DHT:
Group 1: -22±40.60A combination of MN and 0.02% DST was able to significantly increase hair density and width, as well as improve the terminal/vellus ratio. Serum DHT was also reduced. Patient-self-assessment was improved however, according to the investigator assessment, there was no change in the Norwood/Hamilton scale. Small sample size, short follow-up period. Group 1:
Pain = 86.67% (13)
Headache = 13.33% (2)
Itching = 33.33% (5)
Group 2:
Pain = 66.67% (10)2Sanchez-Meta et al (2022) n=34 (M)
Group 1: 17
Group 2: 17AGAComparative, double-blind, randomized prospective study. Group 1: MN + topical DST (0.01%)
Group 2: MN only12 treatments (3 every 4 weeks), then follow-up at 16 weeks. 16 weeks GPA using a 4-point rating scale, photo-trichoscopy, pain assessment using VAS GPA:
Group 1: 11.8% mild, 35.3% moderate, and 52.9% marked improvement. Group 2: 47.1%, 35.3%, and 17.6%, respectively (p = 0.037).
Hair diameter from baseline: dutasteride (frontal) 6µm vs 16µm, (occipital) 5µm vs 12µm (p = 0.049).
Hair density from baseline: dutasteride (frontal) 5.5 vs. 26.6 hairs per cm2, (occipital) 5 vs. 12 hairs per cm2 (p = 0.045).
Vellus terminal ratio: (frontal) -0.09 vs -0.38, (occipital) no data. (p = 0.045).MN + DST produces a superior overall change in hair thickness and density compared to MN alone. Small sample size and short treatment duration Erythema and sensitive scalp lasting up to 36 hours affected 88.2% and 84.2% of saline and dutasteride groups, respectively. 2 -
-
FREE RESOURCES
Research Tables
Want the latest research on Mesotherapy Dutasteride? Every quarter, our research team conducts a literature search on Mesotherapy Dutasteride to keep you up-to-date on new studies. See our search criteria & research tables below – including a summary of key findings from every single study.
Last updated: October 2024
Results
Search Criteria
Parameter
Inclusion Criteria
Exclusion Criteria
Patients Patients of any age with hair loss. Patients with no hair loss disorder. Intervention Mesotherapy dutasteride as a standalone or adjunct therapy. A study that doesn’t contain mesotherapy dutasteride either as a standalone or adjunct therapy. Comparator Placebo and/or other therapies or baseline. No comparator. Outcomes Primary Endpoints of phototrichogram, investigator, and/or patient or physician assessments. None. Study Design Prospective, observational, retrospective, and case series studies. Literature reviews, non-human subjects, or ongoing clinical trials. Search Terms
Search Terms:
dutasteride mesotherapy intradermal intralesional alopecia hair loss-
Abbreviations:
-
FPHLFemale pattern hair loss
-
GPAGlobal Photographic Assessment
-
DSTDutasteride
-
MetSMetabolic syndrome
-
OMOral minoxidil
-
MXMinoxidil
Summarized Studies
Study Participants Design Treatment Results Key Takeaway Adverse Effects Evidence Quality Authors (year) Sex Hair Loss Type Design Treatment Types Treatment Regimen Procedure No. of Sessions Duration Endpoints Hair Growth Assessments Summary Limitations Adverse Effects Jadad Score Moftah et al (2021) n=51 (F)
Group 1: 26 (with FPHL + MetS)
Group 2: 25 (without FPHL + MetS)
 FPHL
FPHL
with MetS
Prospective cohort study 0.02% DST injections Weekly for 12 weeks, then every 8 weeks for 32 weeks. Intradermal injection in a defined area of the vertex by 0.05 ml at 2 cm interval using a 30-gauge needle with 30° angle. 16 47 weeks Trichoscopy, Investigator assessment, patient self-assessment, evaluation of side effects 3 months post - treatment:
% of Terminal hair =
Group 1: 70.86%±11.95
Group 2: 86.04%±6.17
% Vellus hair = Group 1: 29.29%±12.02
Group 2: 14.45%±5.98
Mean Hair Thickness:
Group 1: 0.024 mm±0.009
Group 2: 0.033 mm±0.007
Investigator Assessment: Group 1: 0.9±0.91 (stabilization)
Group 2: 1.9±0.91 (slight improvement).MetS negatively impacted response to intradermal injection of DST for patients with FPHL. Small sample size, short follow-up period. None were reported in either group. 2Saceda-Corralo et al (2017) n=6
(M = 5)
(F =1)AGAProspective clinical study 0.01% DST Every 3 months Not reported 3 24 weeks with assessments taking place 36 weeks after the last session Serum hormone tests and trichoscopuy Serum Hormone: No differences were observed before and after treatment.
Trichoscopy: Increase in hair density and diameter observed.DST intradermal injection may be an effective therapy for patient with AGA, even with less intensive treatment schedules. Small sample size, No raw data given for hair counts. No adverse effects recorded. 1Moftah et al (2013) n= 126 (F).
Group 1: 86
Group 2: 40FPHLPlacebo controlled, open, randomized, prospective study. Group 1: 2 mL of 0.05% DST solution.
Group 2: 2 mL of saline.Weekly for 8 weeks, then weeks 10, 12, and 16. Intradermal injection of vertex by 0.05 ml solution at a 1 cm interval at a 2-4 mm depth at an angle of 30-60° using a 4 mm long 30 gauge needle. 11 16 weeks GPA using a 6-point rating scale, week, hair pull (with epilated hair count), hair strand diameter, and patient self-assessment. Five patients were also given ultrastructural examinations. GPA: improvement in 62.8% of the treatment group (30.2% mild, 15.1% excellent) (p <0.05). For the control group 17.5% of users showed mild improvement.
Hair number in the hair pull test at baseline: 5.2 ± 1.2 vs 3.8 ± 1.7 at week 18 in the treatment group and 4.7 ± 1.5 in the control group (p < 0.05).
Hair Diameter: 25.8 ± 7.6 µm, vs 34.6 ± 11.8 µm in the treatment group compared to 26.8 ± 3.8 µm in the control group (P < 0.05).
Patient self-assessment: Improvement more significant in group 1 than group 2 (p < 0.05).
Ultrastructural examination: revealed return of cuticle or repair.DST intradermal injection was effective, tolerable, and minimally invasive treatment modality in FPHL. Did not count the number of terminal hairs per follicular unit. Tolerable pain in both groups (82.6% and 80% respectively). Headaches reported in 22.1% and 12% respectively (up to 1 per day). Itching in 3.5% and 0% respectively. 3Sobhy et al (2013) n=90 (M)
Group 1: 30
Group 2: 30
Group 3: 30AGARandomized clinical trial Group 1: DST 0.05%
Group 2: DST 0.05%, dexpanthenol 500 mg, biotin 20 mg, pyridoxine200 mg
Group 3: 0.9% saline.Once weekly for four weeks then once every two weeks for four weeks, then once every four weeks for 12 weeks. Not reported 9 19 weeks Trichogram analysis, investigator assessment, patient self-assessment, semenogram, and serum DHT. Trichogram:
Results favored Group B, showing statistically significant increases in anagen hair %, hair shaft diameter and anagen/telogen ratio.
Patient satisfaction:
Patients in Group 1 and 2 reported high levels of satisfaction.
Semenogram: Group 1: Decline in semen volume + sperm motility
Group 2: Decline in sperm concentration + sperm motility. No change in sperm morphology between any of the groups.The DST-containing mixture (Group 2) appears to exhibit the highest efficacy for hair growth, however, further studies should be completed to investigate systemic absorption. Needs further research to examine potential systemic effects. Semen parameter changes. 3 -
- Mission Statement