- About
- Mission Statement
Education. Evidence. Regrowth.
- Education.
Prioritize knowledge. Make better choices.
- Evidence.
Sort good studies from the bad.
- Regrowth.
Get bigger hair gains.
Team MembersPhD's, resarchers, & consumer advocates.
- Rob English
Founder, researcher, & consumer advocate
- Research Team
Our team of PhD’s, researchers, & more
Editorial PolicyDiscover how we conduct our research.
ContactHave questions? Contact us.
Before-Afters- Transformation Photos
Our library of before-after photos.
- — Jenna, 31, U.S.A.
I have attached my before and afters of my progress since joining this group...
- — Tom, 30, U.K.
I’m convinced I’ve recovered to probably the hairline I had 3 years ago. Super stoked…
- — Rabih, 30’s, U.S.A.
My friends actually told me, “Your hairline improved. Your hair looks thicker...
- — RDB, 35, New York, U.S.A.
I also feel my hair has a different texture to it now…
- — Aayush, 20’s, Boston, MA
Firstly thank you for your work in this field. I am immensely grateful that...
- — Ben M., U.S.A
I just wanted to thank you for all your research, for introducing me to this method...
- — Raul, 50, Spain
To be honest I am having fun with all this and I still don’t know how much...
- — Lisa, 52, U.S.
I see a massive amount of regrowth that is all less than about 8 cm long...
Client Testimonials150+ member experiences.
 Scroll DownPopular Treatments
Scroll DownPopular Treatments- Treatments
Popular treatments. But do they work?
- Finasteride
- Oral
- Topical
- Dutasteride
- Oral
- Topical
- Mesotherapy
- Minoxidil
- Oral
- Topical
- Ketoconazole
- Shampoo
- Topical
- Low-Level Laser Therapy
- Therapy
- Microneedling
- Therapy
- Platelet-Rich Plasma Therapy (PRP)
- Therapy
- Scalp Massages
- Therapy
 More
More
IngredientsTop-selling ingredients, quantified.
- Saw Palmetto
- Redensyl
- Melatonin
- Caffeine
- Biotin
- Rosemary Oil
- Lilac Stem Cells
- Hydrolyzed Wheat Protein
- Sodium Lauryl Sulfate
 More
More
ProductsThe truth about hair loss "best sellers".
- Minoxidil Tablets
Xyon Health
- Finasteride
Strut Health
- Hair Growth Supplements
Happy Head
- REVITA Tablets for Hair Growth Support
DS Laboratories
- FoliGROWTH Ultimate Hair Neutraceutical
Advanced Trichology
- Enhance Hair Density Serum
Fully Vital
- Topical Finasteride and Minoxidil
Xyon Health
- HairOmega Foaming Hair Growth Serum
DrFormulas
- Bio-Cleansing Shampoo
Revivogen MD
- more
Key MetricsStandardized rubrics to evaluate all treatments.
- Evidence Quality
Is this treatment well studied?
- Regrowth Potential
How much regrowth can you expect?
- Long-Term Viability
Is this treatment safe & sustainable?
Free Research- Free Resources
Apps, tools, guides, freebies, & more.
- Topical Finasteride Calculator
- Interactive Guide: What Causes Hair Loss?
- Free Guide: Standardized Scalp Massages
- 7-Day Hair Loss Email Course
- Ingredients Database
- Interactive Guide: Hair Loss Disorders
- Treatment Guides
- Product Lab Tests: Purity & Potency
- Evidence Quality Masterclass
- More
Articles100+ free articles.
-
Cannabidiol (CBD) Increases Hair Counts By 246%? Not So Fast.
-
Creatine: Does It Worsen Hair Loss? It Depends On The Hair Loss Type.
-
Can Progesterone Improve Hair Regrowth?
-
CRABP2: Can This Gene Predict Regrowth From Retinoids?
-
BTD: Can This Gene Predict Regrowth From Biotin?
-
COL1A1: Can This Gene Predict Regrowth From Collagen Support?
-
2dDR For Hair Loss: What Do We Know So Far About This Sugar?
-
CYP19A1: Can This Gene Predict Regrowth From Hormone Therapy?
PublicationsOur team’s peer-reviewed studies.
- Microneedling and Its Use in Hair Loss Disorders: A Systematic Review
- Use of Botulinum Toxin for Androgenic Alopecia: A Systematic Review
- Conflicting Reports Regarding the Histopathological Features of Androgenic Alopecia
- Self-Assessments of Standardized Scalp Massages for Androgenic Alopecia: Survey Results
- A Hypothetical Pathogenesis Model For Androgenic Alopecia:Clarifying The Dihydrotestosterone Paradox And Rate-Limiting Recovery Factors
Menu- AboutAbout
- Mission Statement
Education. Evidence. Regrowth.
- Team Members
PhD's, resarchers, & consumer advocates.
- Editorial Policy
Discover how we conduct our research.
- Contact
Have questions? Contact us.
- Before-Afters
Treatments-

Evidence Quality
73%
Regrowth Potential
Long-Term Viability
Written by Perfect Hair Health TeamMedically Reviewed by Rob EnglishFirst Published Oct 6, 2024Last Updated Oct 24, 2024Key Information
Free Resources
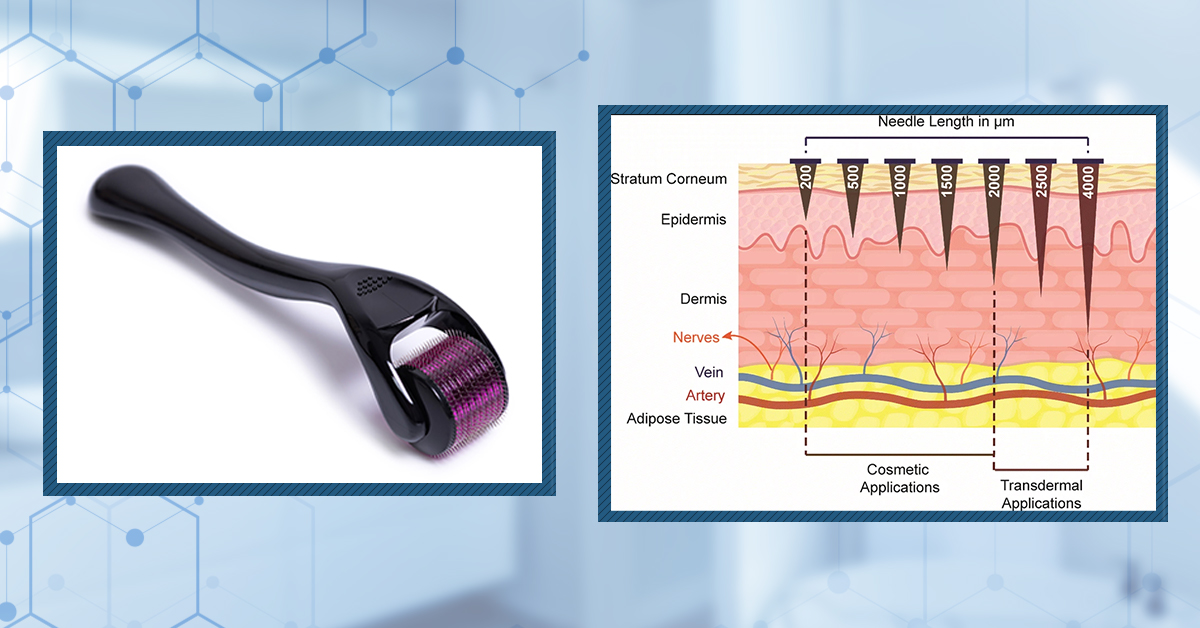
KEY INFORMATIONWhat Is Microneedling?
Microneedling is a therapy that involves the deliberate and repeated wounding of skin – often at depths of 0.25mm to 5.0mm. It can be administered at-home or by a medical professional.
How Does Microneedling Work?
Microneedling is believed to work through mild acute inflammation, which then releases growth factors that may improve skin scarring, increase angiogenesis (new blood vessel networks), and initiate new hair cycles.
What You Should Know
Research on microneedling is limited. However, clinical studies currently suggest that microneedling appears to enhance hair growth, and that it might enhance the hair growth-promoting effects of other topicals – such as minoxidil – by up to 400%.
FREE RESOURCESArticles
Explore the science behind hair loss and hair growth. Our in-depth articles cover topics ranging from natural remedies to pharmaceuticals to breakthroughs in hair loss science. Want to request an article topic? Contact us.
 By Sarah King, PhDMay 31, 2024
By Sarah King, PhDMay 31, 2024Microneedling the Scalp: Does it Cause Scarring?
Can repeated microneedling on the scalp cause scarring? There aren’t yet long-term studies answering this question. On the one hand, microneedling increases neocollagenesis (i.e., the formation of new collagen, or skin tissue). On the other hand, studies show that microneedling-induced collage... By Perfect Hair Health TeamApr 25, 2024
By Perfect Hair Health TeamApr 25, 2024Why Am I Shedding After Microneedling?
Temporary hair shedding is commonly reported after men & women start hair loss treatments like minoxidil. But is temporary hair shedding also normal when starting microneedling? On the one hand, microneedling induces acute inflammation. A little inflammation might benefit hair growth, while too ...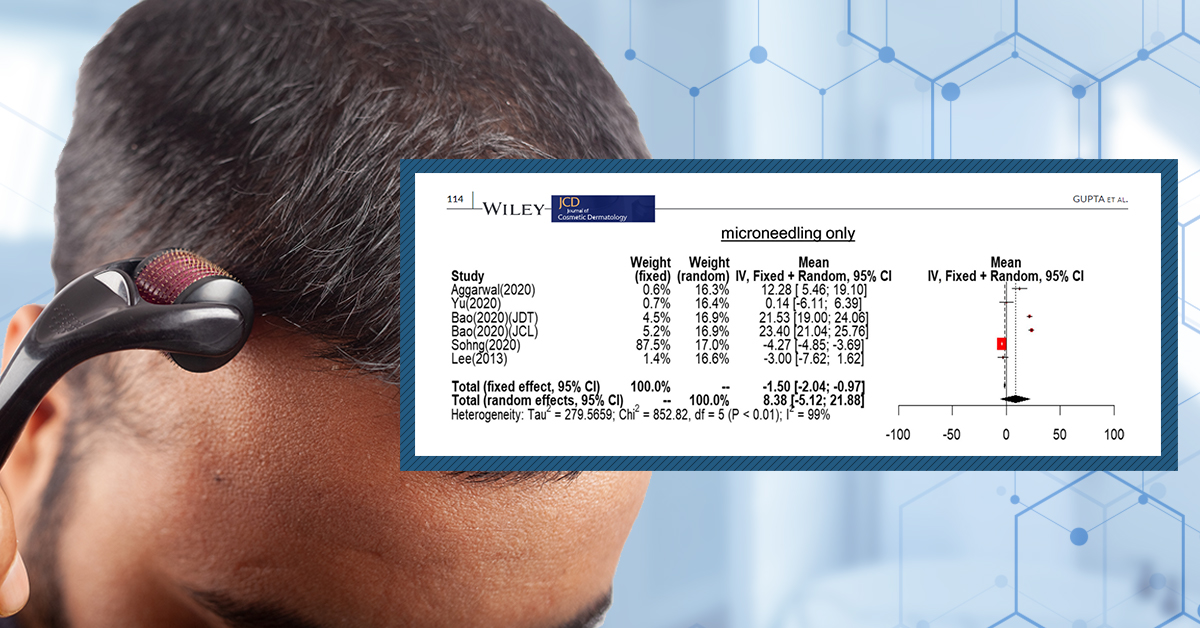 By Sarah King, PhDApr 19, 2024
By Sarah King, PhDApr 19, 2024What Happens If I Stop Microneedling?
In general, treatments for hair loss are only effective as long as they are continued. However, limited data suggests that microneedling may exert its effects up to six months post-treatment (with or without minoxidil). In this article, we will dive into the research behind how long the positive hai...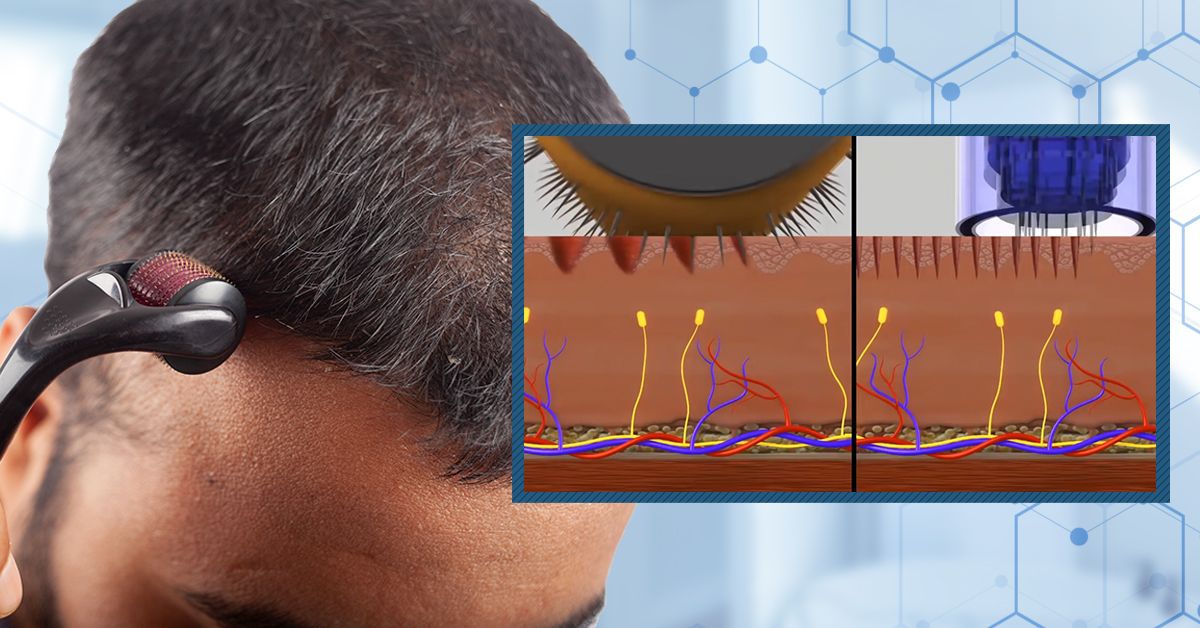 By Rob EnglishApr 11, 2024
By Rob EnglishApr 11, 2024Am I Supposed to Bleed When Microneedling? A Scientific Analysis
Microneedling is an experimental hair loss intervention that creates tiny punctures on the scalp skin surface – which improves topical penetration and triggers the body’s natural healing response. During a microneedling session, it’s normal to experience a bit of pinpoint bleeding. Havin... By Rob EnglishApr 11, 2024
By Rob EnglishApr 11, 2024Microneedling vs PRP: Which Is Better?
Dermatologists often recommend platelet-rich plasma therapy (PRP) as a treatment for hair loss. However, studies suggest that microneedling might also achieve the same results for a fraction of the price. This article provides a comprehensive comparison of PRP versus microneedling: the clinical evi...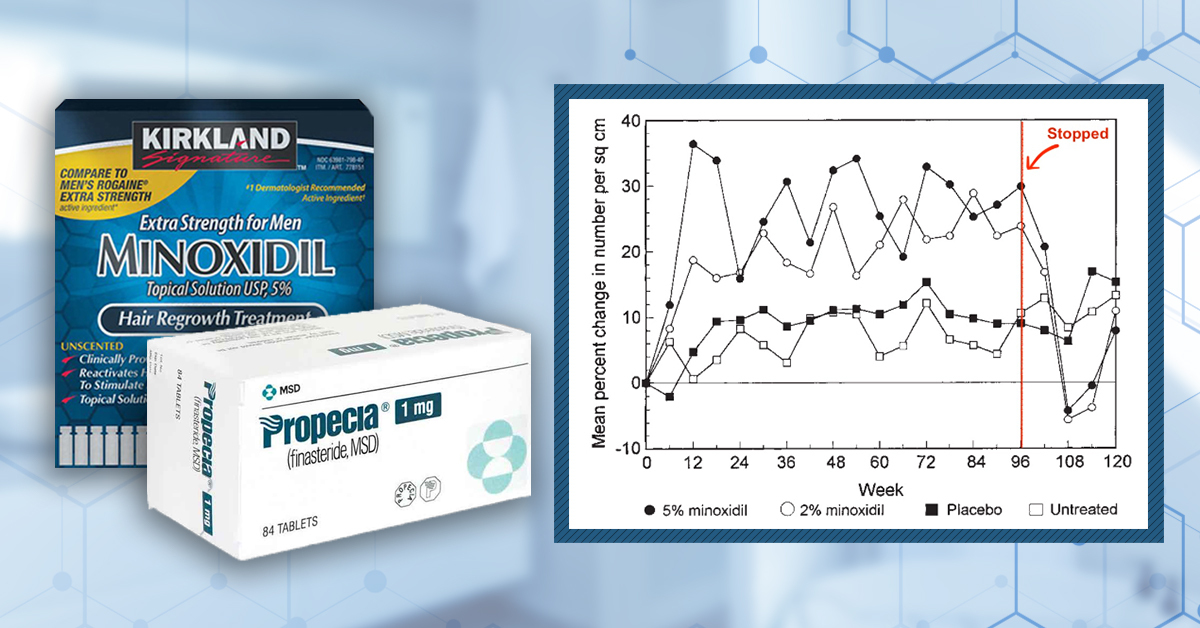 By Sarah King, PhDApr 11, 2024
By Sarah King, PhDApr 11, 2024Is Hair Loss Treatment Lifelong? Here’s What The Data Show.
It can be daunting to think of hair loss treatments as a lifelong commitment. And for most cases of androgenic alopecia, this is true. However, starting treatment does not necessarily mean you must commit to a lifetime of treatment. Studies suggest that after stopping a hair loss treatment, hair los... By Perfect Hair Health TeamJan 10, 2023
By Perfect Hair Health TeamJan 10, 2023Microneedling Infection: Is the Scalp at Risk?
Microneedling is a popular way to combat hair loss and promote hair growth. It creates low levels of inflammation in the scalp tissue, which triggers an adaptive response in the body; growth factors and signaling proteins are recruited for wound repair. However, as with any wound (no matter how smal... By Perfect Hair Health TeamSep 16, 2022
By Perfect Hair Health TeamSep 16, 2022Microneedling For Hair Loss: 5 Strategies to Reduce Pain
Microneedling is an experimental therapy for androgenic alopecia and other hair loss disorders. One of its downsides is that it is painful to administer. However, there are simple and effective strategies to reduce pain levels while microneedling across the scalp:(1) opting for devices that ensure n... By Perfect Hair Health TeamApr 10, 2022
By Perfect Hair Health TeamApr 10, 2022Mature Hairline vs Receding: How to Tell the Difference
It can be difficult to distinguish between a mature hairline and a receding hairline. After all, hairline changes are a natural part of the aging process. What key characteristics separate hairline maturation from outright recession? This investigative post will explain 1) How to identify a mature h...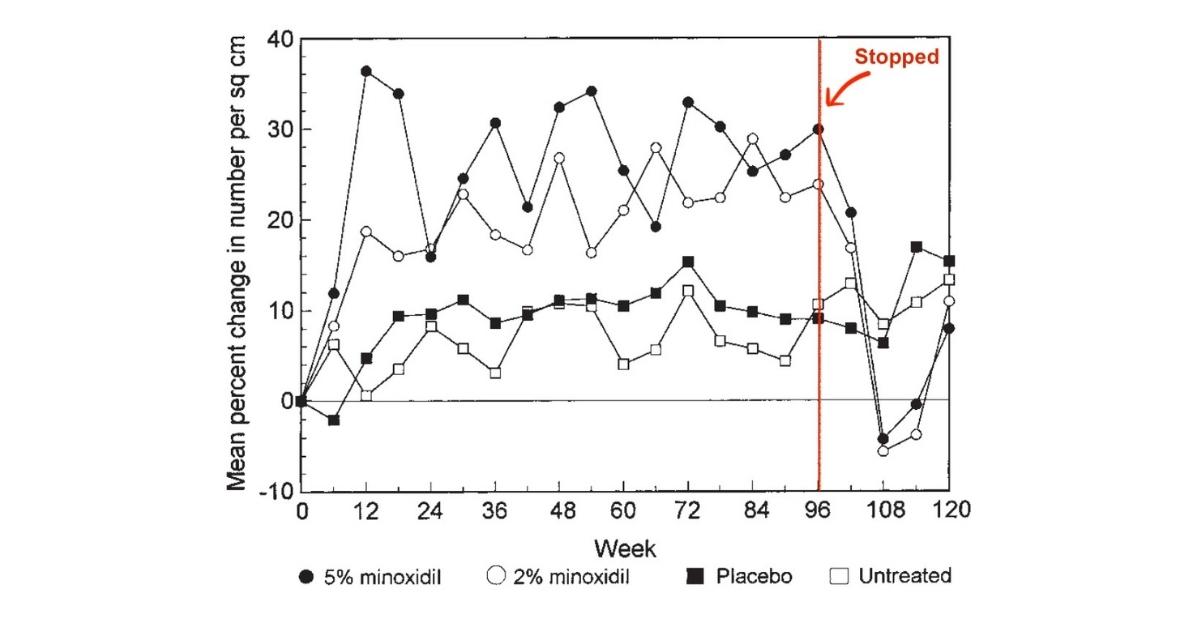 By Perfect Hair Health TeamMar 10, 2022
By Perfect Hair Health TeamMar 10, 2022How Long After Stopping Minoxidil Before We Lose Our Hair Gains?
Studies show that within 3 months of quitting minoxidil, any new hair growth is lost and, worryingly, our hair loss temporarily worsens before returning to baseline. But encouragingly, new studies are revealing potential ways to mitigate any shedding related to minoxidil withdrawals. In fact, a 2020... By Perfect Hair Health TeamMar 5, 2022
By Perfect Hair Health TeamMar 5, 2022Three Ways to Improve Minoxidil Results
Minoxidil is one of the most widely used hair loss products on the market. And yet, so much about this growth activating “pro-drug” remains unknown. Despite its FDA approval, results are not guaranteed. In fact, around 50% of hair loss sufferers are non-responders. Recent research sugges... By Perfect Hair Health TeamJul 2, 2020
By Perfect Hair Health TeamJul 2, 2020Scarring Alopecias: What Makes Them Unique (And Reversible)
Scarring alopecias were once thought to be irreversible. Now, studies are proving just the opposite. Case reports are showing that people with scarring alopecias have experienced complete hair regrowth, and from changes as simple as quitting sunscreen. Read on to learn the science behind these scarr... By Perfect Hair Health TeamJan 16, 2020
By Perfect Hair Health TeamJan 16, 2020Microneedling For Hair Loss: Daily, Weekly, Or Bi-Weekly?
Clinical studies show that microneedling once every 1-3 weeks helps to regrow hair. Then again, 1-3 week intervals are the only frequencies studied for pattern hair loss. With men on hair loss forums reporting amazing results from microneedling as often as once per day, could we be missing something... By Perfect Hair Health TeamJan 7, 2020
By Perfect Hair Health TeamJan 7, 2020Microneedling For Hair Loss: What’s The Best Needle Size?
When it comes to microneedling for hair regrowth, researchers aren’t yet sure which needle size elicits the best results. In clinical studies, needle lengths of 0.6mm to 2.5mm (used once weekly or bi-weekly) have been shown to improve hair counts in men with androgenic alopecia (AGA). Even sti...-
FREE RESOURCES
Research Tables
Want the latest research on Microneedling? Every quarter, our research team conducts a literature search on Microneedling to keep you up-to-date on new studies. See our search criteria & research tables below – including a summary of key findings from every single study.
Last updated: October 2024
Results
Search Criteria
Parameter
Inclusion Criteria
Exclusion Criteria
Patients Patients of any age treated for scalp hair loss. Patients with no hair loss disorder. Intervention Microneedling as a standalone or adjunct therapy. Acupuncture needles or microneedling devices with needle-releasing drugs. Comparator Placebo and/or other therapies or baseline. No comparator. Outcomes Primary Endpoints of phototrichogram, investigator, and/or patient assessments. Any study not designed to adequately test for the standalone or additive effect of microneedling. Study Design Prospective studies. Literature reviews, non-human subjects, or ongoing clinical trials. Search Terms
Search Terms:
microneedling areata hair loss cicatricial effluvium microneedle alopecia-
Abbreviations:
-
FPHLFemale pattern hair loss
-
AGAAndrogenetic alopecia
-
AAAlopecia areata
-
MXMinoxidil
-
MNMicroneedling
-
PRPPlatelet-rich plasma
-
TATriamcinolone acetonide
-
MXTTopical minoxidil
-
AUAlopecia Universalis
-
ATAlopecia Totalis
-
AASISAlopecia Areata Symptom Impact Scale
-
SALTSeverity of Alopecia Scoring Tool
-
FGFFibroblast growth factor
-
SPTSpironolactione
-
LADLesional Hair and Density Score
Summarized Studies
Study Participants Design Treatment Results Key Takeaway Adverse Effects Eq Authors (year) Sex Hair Loss Type Design Treatment Types Treatment Regimen MN Procedure No. of Sessions Duration Endpoints
Hair Growth Assessments Summary
Limitations
Adverse Effects Jadad Score Zhang et al (2022) n=40 (F)
Group 1 = 20
Group 2 = 20 FPHL
FPHLSingle-center, randomized, controlled, evaluator-blinded clinical trial. 2% MXT and MN. Group 1: 2% MXT alone.
Group 2: 2% MXT + MN.MN length of 260 μm. Two passes until the scalp becomes reddish. 2% MX was then applied. Group 1: twice daily
Group 2: twice daily MXT with once weekly MN.24 weeks Investigator assessment of hair growth and change from baseline hair counts. Effective rate in Group 2 was 85% which was significantly higher than that of Group 1(45%). Hair counts were also higher in the combined treatment group. MN combined with MXT had better efficacy for FPHL during treatment and follow-up Small sample size, single-center study, lack of placebo control, short-follow-up period. Group 1: Hirsutism = 3
Scalp itching and transient increase in hair loss = 7
Group 2: Occasional headache = 2
Hirsutism = 10
Scalp itching and transient increase in hair loss = 1
2El Mulla et al (2022) n=60
Group 1: 15 (M:6, F:9)
Group 2: 15 (M:9, F:6)
Group 3: 15 (M:6, F:9)
Group 4: 15 (M:10, F:5) AA
AAInterventional, comparative study. Fractional carbon dioxide laser, TA, MN and PRP. Group 1: Fractional carbon dioxide laser + TA (10 mg/mL).
Group 2: MN and TA (10 mg/mL).
Group 3: Fractional carbon dioxide laster + PRP.
Group 4: MN + PRP.Dermapen with a 36-needle tip 2 - 2.5 mm long needle depth used until pinpoint bleeding or mild erythema occurred. Every 3 weeks. 12 weeks with a follow-up four weeks later. Hair regrowth assessment (SALT scores), improvement scores, and dermascopic changes. At the four-week follow-up: 80% of patients in group 2 improved SALT score to 0 (no hair loss), whereas group1 and group 4 improved by 40%. Group 3 improved only 13.3%.
Hair regrowth scores showed that group 2 showed maximum improvement with 80% of patients scoring RGS5.
Overall, the MN + TA group showed the most significant improvement. Small sample size, no blinding. No major complications were observed, but heat discomfort was reported during CO2 laser procedures. 2Abdallah et al (2022) n=20
M:19
F:1
AAProspective, intra-patient controlled study. TA, MX, MN or nothing. Patch 1: Intralesional TA.
Patch 2: intradermal MX.
Patch 3: Combined intradermal TA + MX.
Patch 4: MN.
Patch 5: Negative control.ZGTS Titanium derma roller. 4-5 passes longitudinally, vertically, and diagonally. Every four weeks 16 weeks SALT score and lesional area density (LAD) score. Trichoscopy and photographic documentation to evaluate treatment response. SALT and LAD scores decreased in patches 1, 2, 3, and 4; the largest differences were seen in patches 1 and 3 vs. patch 5. Intradermal injection did not show significant superiority over spontaneous regrowth in patchy non-severe AA suggesting that microneedling may be a comparable option. Short treatment duration, small sample size. Mild burning pain reported during the procedure, but treatment was generally tolerable.
No serious adverse events recorded.
2Abd ElKawy et al (2022) n=30
(M:18, F:12)
AAProspective, split-side, comparative study. Fractional CO2 laser, TA, and MN. Side 1: Fractional CO2 laser + TA.
Group 2: MN + TA.Side 2: 12-needle cartridge at a depth of 1.5 mm until pinpoint bleeding and erythema were observed. Every four weeks. 24 weeks Clinical response, efficacy and safety, dermoscopic imaging, and SALT score. Side 1: 56.7% achieved complete response, 23.3% partial response, and 20% no response.
Side 2: 86.7% achieved complete response, 6.7% partial response, and 6.7% no response.
Side 2 showed better clinical response and SALT score improvement. Dermoscopic signs improved significantly in both groups. Duration of AA influenced response and no. of sessions needed for improvement.
While both treatments proved effective for treating AA, MN demonstrated better results and was more tolerable. Small sample size, not controlled, short follow-up period. Mild pain and erythema in a few patients. 3Muhammad et al (2022) n=60
Group 1: 30 (M:27, F:3)
Group 2: 30 (M) AGA
AGARandomized, observational, interventional study. PRP and MN. Group 1: P
RP alone.
Group 2: MN + PRPGroup 2: derma roller with needles measuring 2 mm until erythema and pinpoint bleeding were observed. PRP was then applied. Every four weeks 12 weeks Photographs of the scalp, hair pull test to assess hair loss, hair count in a predefined 1 cm2 area of the scalp, and patient-reported levels of satisfactions using a Likert scale. Negative Hair Pull Test:
Group 1: 51.9%, Group 2: 82.1%.
Improved Perception of Hair Loss: Group 1:73.9%
Group 2: 88%.
% increase in hair count:
Group 1: 17.88±10.15%, Group 2: 24.53±9.49% (p = 0.011).MN + PRP was found to have better treatment outcomes, increased hair count, and lower pain perceptions compared to PRP alone. Patients receiving combined treatment reported higher satisfaction and lower pain scores. The combined approach may offer improved treatment success rates, patient satisfaction, and compliance. Small sample size, underrepresentation of female participants, no control group. None mentioned. 1Arora et al (2022) n=60 AGAProspective, randomized, comparative study. MN and TA Group 1: MN with local application of injectable TA.
Group 2: Injectable TA administered intradermally.Group 1: dermaroller of needle size 1.5 mm was moved on the scalp patches 4-5 times in each direction until pinpoint bleeding was observed.
Group 2: Intradermal injections of 10 mg/mL TA with a disposable insulin syringe.Once every 3 weeks 9 weeks Clinical examination, area measurement of patches, regrowth evaluation, uniformity of regrowth, and adverse effects. Both groups showed significant regrowth. Group 1: exhibited mean regrowth of 66.36% at week 9.
Group 2: exhibited mean variegated regrowth of 69.75% at week 9.Injectable TA used with MN and intralesionally has similar efficacy in promoting hair regrowth in AA. MN resulted in more uniform but less dense regrowth. Small sample size, short follow-up, lack of patient feedback evaluation Group 1: Tinea infection = 1.
Group 2: Hypopigmentation = 2.2Liang et al (2022) n=120 (F)
Group 1 = 38
Group 2 = 37
Group 3 = 40FPHLProspective, single-cente, parallel-group, evaluator blinded, randomized trial. MXT, spironolactone (SPT), and MXT + MN. Group 1: 5% MXT.
Group 2: 80-100mg SPT + 5% minoxidil.
Group 3: 5% MX + MNElectrodynamic microneedling inserted at a depth of 0.7 - 1 mm until pinpoint bleeding was observed. Group 1: Once daily.
Group 2: Once daily.
Group 3: Topical MX once daily plus MN every 2 weeks.24 weeks Hair growth, scalp tissue structure, physician and patient assessments, and side effects. MXT + MN group showed the most increased hair density (99.68±15.58 - 130±20.58) and MXT showed the least (101.37±17.32 - 111.32±19.57).
Hair shaft diameter significantly increased in all groups. Epidermal thickness and average hair follicle diameter increased only in the MXT + MN group. Dermis thickness increased in all groups. Both physician’s and patient’s assessments showed improvement in all three groups.
The combination of MXT and MN was found to be the most effective choice for treating mild-to-moderate FPHL in women with regular menstrual cycles and normal hormone levels, compared to either MX plus SPT or MX alone. Severe FPHL patients (Sinclair IV and V) were excluded. Unblinded. Group 1: facial hypertrichosis=4, trichomadesis aggravating=4, scalp pruritus=8, increased scurf=7, headache=1, palpitation=1, postural hypotension=1, urticaria=1.
Group 2: facial hypertrichosis=5, trichomadesis aggravating=4, scalp pruritus=8, increased scurf=6, edema=1, headache=1, palpitation=3, hyperkalemia=1, menstrual disorder=15, urticaria=1.
Group 3: facial hypertrichosis=5, trichomadesis aggravating=3, scalp pruritus=9, increased scurf=5, infection=1, postural hypotension=1.4Ozcan et al (2022) n=62 (M) AGARandomized, controlled trial PRP, MN and point-by-point injection. Group 1: PRP + MN
Group 2: PRP + point-by-point injectionGroup 1: 1.5 mm MN.
Group 2: 30 gauge, 5 mm syringe.3 sessions every 2 weeks initially and then a fourth session 1 month later 10 weeks Trichoscan analysis, hair pull test, and patient/physician global assessment scores Both PRP applications showed significant improvements in hair growth parameters (hair count, density, anagen/telogen ratio, and hair length). Hair pull test became significantly negative in both groups, indicating reduced hair loss. Patient and physician satisfaction scores were high in both groups. Whilst both groups showed significant improvements in hair growth parameters, PRP + MN was found to be superior in certain aspects. The lack of a placebo group and limited follow-up period. None mentioned. 1Bao et al (2022) n=71 (M)
Group 1: 23
Group 2: 23
Group 3: 25AGARandomized, controlled trial. 5% MXT, and electrodynamic MN treatment Group 1: 5% MXT
Group 2: Electrodynamic MN
Group 3: Combination MXT and MN.Groups 2 and 3: MN device inserted at a depth of 1-2 mm Group 1: Applied twice daily.
Group 2: MN every 3 weeks.
Group 3: MXT twice daily + MN every 3 weeks.24 weeks + 24 weeks follow-up Phototrichography to measure growth, thickness and density. Evaluation every 3 weeks and details of any toxicities related to treatments were collected. All three groups showed a significant increase in non-vellus hair density after treatment. Group 3: showed the highest increase in non-vellus hair density (22.46±3.87). Group 3: showed the more superior final hair density (39.78±7.79). Vellus hair density decreased in groups 1 and 3 after treatment, but not in group 2. Final hair diameter increased significantly in groups 1 and 3.
Follow up: Group 3: maintained the increased hair density. Group 1: Hair loss recurred.
MN combined with MXT can effectively treat AGA and promote hair growth. Small sample size, only the combination group received scalp massages after treatment, which may confound the results. Group 1: seborrheic dermatitis, scalp itching, and eczema.
Group 2: increased dandruff, scalp infection and enlarged lymph nodes.
Group 3: seborrheic dermatitis, increased dandruff, and enlarged lymph nodes.3Aboeldahab et al (2021) n=80
Group 1: 40 (F:16, M:24)
Group 2: 40 (F:14, M:26)AAProspective, randomized, single-blinded trial. Superficial cryotherapy + MN Group 1: Superficial cryotherapy
Group 2: MNDermapen for 4-5 passes in each direction. Needle range from 1-2 mm. Every 2 weeks. 12 weeks with follow-up 12 weeks later. SALT score, trichoscopy, AASIS for patient self-assessment. Both treatments showed improvements in the SALT score and hair density. Group 2 showed slightly better results in terms of SALT score change and hair density change percentages. Good to excellent responses were achieved in both groups, with microneedling showing a slightly higher rate of success. No recurrence of AA was observed in responders of either group during the follow-up period. Both superficial cryotherapy and MN are effective and well-tolerated options for mild scalp AA. MN demonstrated slightly better efficacy. Only mild AA cases used, with no control group. Transient adverse effects were reported in the cryotherapy group, while the MN group did not report any significant side effects. 3Burns et al (2021) n=11 (F) FPHLPilot, interventional study. Combination 5% MXT + MN added to ongoing hair loss treatments. Combination 5% MXT + MN added to ongoing hair loss treatments. MN automated pen, session endpoints marked as two passes across the frontal, crown, vertex, and upper-parietal scalp. Every 2 weeks. 12 weeks Photographic evaluation, self assessments Investigators noted that 11/11 subjects improved at lease 1-1,5 Sinclair scores. Combination MXT + MN appears to be an effective treatment for FPHL. Small sample size, no placebo or comparator, short study length. Transient headache, pinpoint bleeding, and mild erythema.No serious adverse events were reported. 1Ramadan et al (2021) n= 126
(M:46,
F:80)
Group 1: 42.
Group 2: 42
Group 3: 42AGASingle-blind, randomized, controlled study. Combination PRP, 5% MXT, 2.5 mg finasteride (men), 200 mg SPT (women) Group 1: medications + PRP injections
Group 2: medications + MN + topical PRP
Group 3: medications alone.MN automated pen, 2 mm needles, session endpoints marked as 3 passes followed by PRP. Once monthly
24 weeks.
Hair counts, diameters and photographic evaluation. Hair density increased in Group 2 vs. Group 1; larger effect for Groups 1 and 2 versus Group 3. Combination of MN, medications and topical PRP appear to be more beneficial for hair growth in people with AGA. Lack of devices to measure trans-epiermal delivery of growth factors in PRP. No serious adverse events were recorded. Transient pain after PRP = 23 2Gowda et al (2021) n= 90
Group 1: 30
Group 2: 30
Group 3: 30AGAProspective, comparative, parallel-group interventional study. MXT, MN, and PRP Group 1: MXT alone.
Group 2: MXT + MN.
Group 3: MXT + PRP.1.5 mm sized needles were used until pin point bleeding was obseerved. Group 1: twice daily.
Group 2: twice daily MXT with MN once monthly.
Group 3: twice daily MXT with PRP once monthly.16 weeks. Investigator assessment (5-point scale), global phtoographic assessment (7-point scale), and visual andalogue scale (VAS).
Hair counts and dermascopic analysis.
Dermoscopic analysis showed maximum improvement in group 3 (64.37±14.42 - 86.13±14.82), followed by group 2 (69.30±17.97 - 85.73±23.10) While PRP + MXT showed the highest efficacy, it also showed the highest number of adverse effects. Therefore, it may be more beneficial to use MN + MXT. Short study duration. Side effects reported including pain, erythema, burning, and edema. Group 3 reported more side effects than the other groups. 2Shome et al (2021) n=50
(M:25, F:25)
Group 1: 25
Group 2: 25AGAComparative, prospective, single-blind study. Intradermal injection of QR678Neo and QR678Neo + MN. Group 1: Intradermal injection of QR678Neo.
Group 2: MN and then QR678Neo.Group 1: 60 - 70 small injections with 6 mm, 31G needle administered at a depth of 1-2 mm intradermally by nappage technique.
Group 2: Dermaroller with 1.5 mm needle size passed approx. 4-5 times until erythema was observed.Once every 3 weeks. 24 weeks + 24 weeks of follow-up Hair counts, diameters, photographic evaluation, and self-assessment. Hair counts and diameters increased in both groups. However, there was no significant difference between the groups. Whilst there is no significant difference between groups, intradermal injection did appear to show a slightly better outcome in both patient self-assessment and in hair counts. Small sample size, no placebo. Group 1: uncomfortable pain.
Group 2: uncomfortable pain.
Itchy scalp.
Erythema.
2Ragab et al (2020) n=60
Group 1: 20 (F:2, M:18)
Group 2: 20 (F:6, M:14)
Group 3: 20 (F:4, M:16)AARandomized, non-controlled study. PRP, fractional laser therapy, and MN. Group 1: Intradermal PRP injection.
Group 2: fractional laser therapy + topical PRP. Group 3: MN + topical PRP.Dermaroller with 1.5 mm needles was used until mild erythema appeared. Every 4 weeks. 12 weeks. SALT score, and patient satisfaction. Pain during procedures was evaluated using a numeric pain rating scale. All groups showed varying degrees of improvement after treatment sessions. Patients who experienced improvement maintained their progress without recurrence. Pain scores were significantly lower in groups 2 and 3. PRP delivered through each method may benefit hair regrowth in AA patients. MN has the additional advantage of being less costly than fractional laser therapy. Variation in patient response, and even between lesions, short follow-up period and absence of a control group. Pain during procedures was reported, but other side effects were minimal. 2Giorgio et al (2020) n=41
(M:17, F:24)
AARandomized study MN aminolaevulinic acid (ALA), and photodynamic therapy (PDT) Group 1: MN alone using an electronic pen device.
Group 2: 10% ALA-PDT.
Group 3: Combination MN and ALA-PDT.Electronic MN pen with 1 mm penetration. Every 3 weeks. 18 weeks. % of hair regrowth in treated areas. Evaluation using a 4-point scale. Group 3 showed the best clinical outcomes. Complete hair regrowth was observed in 3 patients, ≥50% improvement in 7 patients and <50% improvements in 6 patients. Group 1 showed no improvement. Group 2 showed varying responses, with some achieving improvement. Combination therapy with ALA-PDT and MN yielded better results for AA compared to individual treatments. A small sample size. Not specified. 1Sohng et al (2020) n=29 (M:24, F:5)
Group 1: 11
Group 2: 9
Group 3: 9AGARandomized, parallel-group, 6-month prospective study. Home-use MN and 5% MXT. Group 1: Home-use MN alone.
Group 2: Home-use MN + 5% MXT.
Group 3: 5% MXT alone.0.25mm long spiral grooved MN. Group 1: twice weekly
Group 2: twice weekly + twice daily
Group 3: twice daily.24 weeks. Hair counts and self-assessments. The patient self-assessment score was higher in Group 2 than in the other 2 groups. However, a statistically significant increase in hair count was not seen in any of the groups compared to the baseline. Whilst combination treatment of MN and MXT510 appeared to lead to better outcomes, there were not statistically significant improvements. Small sample size, small hair count area. No serious adverse events were recorded. Mild and transient pruritus noted in one subject. 2Yu et al (2020) n=40 (M)
AGARandomized controlled trial. Combination: 5% MX, growth factors. Group 1: Nano-MN-assisted normal saline.
Group 2: 5% topical MX.
Group 3: Nano-microneedle-assisted fibroblast growth factor (FGF).
Group 4: Combination of 5% topical MX and nano-MN-assisted FGF.Microneedle roller. Once weekly. 16 weeks. Hair counts, hair diameters, photographic evaluation, self assessments. Hair density significantly increased in groups 2, 3, and 4. Hair diameter significantly improved in groups 2 and 4. Follicular unit density significantly improved in groups 3 and 4. Group 4 showed the most satisfactory results in terms of hair density, diameter and follicular unit density. Combination nano-microneedle assisted FGF and topical minoxidil was safe and effective at treating AGA, resulting in improvements in hair density, diameter, and follicular unit density. Small sample size, short-term study. No serious adverse events were recorded. Three subjects developed mild erythema, which alleviated after 24 hours. 3Aggarwal et al (2020) n=30 (M) AGARandomized, triple-blinded cohort study. MN and PRP. Group 1: MN alone.
Group 2: MN combined with PRP.MN roller: 1.5-2 mm needles with session endpoints marked as gentle rolling until pinpoint bleeding. Once monthly. 24 weeks.
Hair counts, hair diameters, self-assessments. Hair thickness and density increased in both groups 1 and 2, but there was no significant difference between the 2 groups. Patient’s subjective satisfaction scores indicated moderate satisfactions, with most patients reporting a reduction in hair fall. Both treatments were well-tolerated, with mild tingling and aching pain as the most common adverse effects. While combination treatment may provide some benefits in treating AGA, the improvement was not significant enough to make it a preferred choice over microneedling alone. Small sample size, need longer-term follow up. No serious adverse events were reported. 3Fagihi et al (2020) n=60 29 - M
31 - F
AGARandomized, controlled trial. 5% MX and MN Group 1: 5% MX
Group 2: 5% MX + MN
Group 3: 5% MX + MNGroup 2: 1.2 mm needles.
Group 3: 0.6 mm needles.Once every 2 weeks. 12 weeks. Hair counts, hair diameters, photographic evaluation, and patient self-assessments. MX + MN was superior to MX alone in terms of hair count, hair thickness and investigator assessment. MN at a depth of 0.6 mm showed trends of better efficacy compared to 1.2 mm. Microneedling combined with minoxidil was effective in treating AGA, with the 0.6 mm microneedling depth showing potential advantages. The treatment was safe and well-tolerated. Small sample size, variations in baseline hair counts and thickness. More pain reported in Group 2 (1.2 mm needles) than in Group 3 (0.6 mm). 2Yu et al (2018) n=19 (M). AGASplit scalp study. 5% MX and fractional radiofrequency MN. Side 1: 5% MX
Side 2: 5% MX + fractional radiofrequency MN.Side 2: 1.5 mm needles. Once every 4 weeks. 20 weeks. Hair counts, hair diameters, photographic evaluation, self assessment. Hair counts and diameters increased on both sides of the scalp, however, the changes to hair counts and diameters were greater on side 2 vs. side 1. 5% minoxidil + fractional radiofrequency MN appears to be an effective and safe treatment option for AGA. Small sample size, short-term study. No serious adverse events were reported. 3Kumar et al (2018) n=68 (M). AGAHospital-based, prospective, single-observer blinded study. MN and MX. Group 1: MN plus 5% topical MX.
Group 2: 5% MX alone.Dermaroller with a needle length of 1.5 mm used until pinpoint bleeding was observed. Group 1: twice daily application + weekly MNfor four weeks then every 2 weeks for four sessions.
Group 2: twice daily application.12 weeks. Increase in hair count from baseline, and patients’ self-assessment of hair growth using a visual analog scale (VAS). Mean increase in hair count at week 12: Group 1: (12.82±6.82) Group 2: (1.89±8.94). MN + 5% MX is an effective, and promising therapy for AGA, this response were only conserved by continuous use of minoxidil. Small sample size and short follow-up period. Group 1:
Mild pain and discomfort during the procedure.
Group 2: No adverse effects seen.2Dhurat et al (2013) n=100 (M)
Group 1 = 50
Group 2 = 50AGARandomized, comparative, evaluator-blinded study MN and 5% MX. Group 1: MN + 5% MX.
Group 2: 5% MX.Dermaroller with a needle length of 1.5 mm sized needles. 5% MX twice daily with MN weekly, 12 weeks.
Change from baseline hair counts using macrophotographs, patient assessment of hair growth, investigator assessment of hair growth. Hair Count: Mean change in hair count at week 12 was significantly greater for Group 1 (91.4 hairs/cm2) compared to Group 2 (22.4 hairs/cm2).
Investigator Assessment: 80% in Group 1 showed a response of +2 - +3 (increased/greatly increased) on the visual analog scale compared to none in Group 2.
Patient Assessment: 82% in Group 1 reported more than 50% improvement in hair growth. 4.5% in Group 2 reported the same level of improvement.Combination MN with 5% MX may be more effective in promoting hair growth in men with AGA. Short duration, no control group. None mentioned. 3Lee et al (2013) n=11 (F) FPHLSplit-scalp, single-blinded, placebo-controlled, pilot study. Growth factor solution, MN, and normal saline. Side 1: Growth factor topical application followed by MN.
Side 2: Normal saline topical application followed by MN.Dermaroller with a needle depth of 0.5 mm. Once weekly. 5 weeks.
Phototrichogram (hair count), patient satisfaction assessed through questionnaires. Increase of more than 10% in hair shaft count was observed on the treated side compared to baseline. Patient satisfaction scores were also higher for the treated side. Topical application of growth factors alongside MN can enhance hair density in women with FPHL. Small sample size, focused on a specific demographic which may limit the generalizability of the findings. No adverse events recorded. 2Yoo et al (2010) n=8
F = 6,
M = 2
 AT
AT
|
6
 AU
AU
|
2
Pilot, split scalp, comparative study.
Photodynamic therapy (PDT), MN, 5-aminolevulinate (MAL). Side 1: PDT with MAL and MN.
Side 2: PDT with MAL.Dermaroller with a needle depth of 0.5 mm. Every 4 weeks. 12 weeks with a final evaluation at 16 weeks. Photographs taken before each session and 1 month after the final treatment. Dermatologists assessed treatment responses by comparing photographs. Hisstologic changes assessed through biopsies. None of the patients achieved hair regrowth in either the microneedled or non-microneedled areas. Histologic analysis showed no difference in hair follicle density between the microneedled and control areas. PDT with MAL might not be effective for recalcitrant alopecia totalis regardless of MN treatment. Small sample size. Mild pain and erythema which resolved after several days. No serious events reported. 1 -
- Mission Statement